Home Health Virtual Summit 2026

As healthcare delivery rapidly shifts beyond traditional clinic walls, for hospital and health system leaders, the real challenge isn’t whether care moves into the home. It’s how to operationalize, staff, support, and scale high-quality care in decentralized environments without adding complexity or cost.
The Home Health Innovation Summit brought together provider leaders who are actively redesigning care delivery, from in-home clinical teams and mobile programs to hybrid models supported by virtual oversight, to share what’s working in real-world settings.
The Summit featured give speakers from leading health systems who shared how they are delivering care where patients live, examining operational design, managing clinical workflows, improving staffing models, and enabling technology that support safe, efficient, and scalable care in the home.
The event concluded with an interactive roundtable discussion, where all speakers came together to answer audience questions and exchange insights on the future of home-based care delivery.
SPEAKERS











FEATURING


AGENDA
Introduction
Inside Out – A Different Approach to Community Health Interventions
The Modern Visiting Nurse Model
Mobile Care & Community-Based Health Delivery
Scaling Home-Based Care Programs
Primary Care at Home: Transforming Outcomes for Complex Seniors
Roundtable – From Idea to Action: Scaling Care Where Patients Are

Embedding Community Health Workers into Clinical Care
Kelly McCabe shared how Sinai Chicago, a large safety-net health system serving predominantly uninsured and Medicaid patients, has evolved its long-standing community health worker (CHW) model by embedding CHWs directly into clinical workflows. Rather than operating solely in the community, CHWs now work alongside care teams in the ED, inpatient units, behavioral health, oncology, and perinatal services, providing culturally concordant support, screening for social needs, and ensuring continuity from admission through post-discharge. Kelly emphasized that integrating CHWs within hospital walls has strengthened care coordination, improved staff buy-in, and surfaced patient needs that might otherwise go unaddressed, reinforcing CHWs as essential members of the care team, not an add-on.

“We want to ensure that there is a seamless continuum of care from the ED to inpatient admission, and then to post-discharge support.”

Scaling Home-Based Advanced Care Through Facilitated Virtual Exams
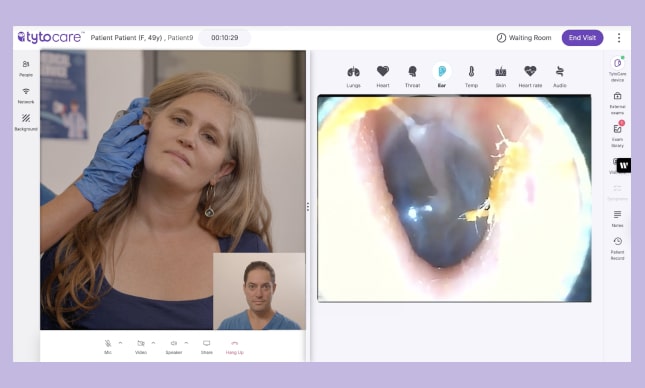
Debra Corbett shared how VNS Health, one of the country’s oldest and largest community-based health organizations, supports medically complex, predominantly geriatric members through a full continuum of care management, from transitions of care to long-term, palliative, and advanced illness support. She walked through the team-based model (nurses, NPs, social workers, pharmacists, care coordinators, 24/7 nurse line) and how VNS uses risk stratification and predictive algorithms to proactively identify members who may benefit from palliative care or hospice. The headline innovation: to solve NP shortages and low visit productivity, VNS created a “facilitated physical exam” model where trained medical assistants conduct in-home visits using a TytoCare kit while a nurse practitioner joins remotely`, allowing the same clinical coverage with more throughput, less travel, and expanded access in underserved areas.

“We were able to solve the lack of capacity to address some underserved areas in New York State, and also to ensure health coverage and equity, in the areas served by VNS Health Plan and the VNS provider organization.”


Designing Trust-Centered Mobile Care for Hard-to-Reach Populations
Dr. James Powell shared how DocGo designs and delivers mobile and virtual care programs that actually work for hard-to-reach populations, especially Medicaid, Medicare Advantage, and dual-eligible members who haven’t seen a provider in a year, drift in and out of care, or rely on the ED as their default. He walked through DocGo’s operating model as “bringing an office into the home,” combining in-home clinicians with remote providers and diagnostic tech to deliver acute, chronic, and preventive care in one coordinated workflow. A big emphasis of his talk was the human side: outreach that earns trust (down to scripts and postcards), a “triangle of care” that includes the patient, provider, and caregiver, and an exam experience built around warmth, soft skills, and clinical rigor, so patients feel safe letting care into their home and clinicians feel confident making decisions outside a traditional clinic.

“We want to think about the patient through what we call a triangle of care. We think about the patient, the provider, and the caregiver. So all our workflows, all our designs, all our documentation, all our education is conscious of all three of those people.”


Scaling Virtual Care Through Simplicity, Integration, and Follow-Through
Tyler Okoren shared how Sentara scaled virtual care by obsessing over one thing: making it simple and truly integrated into the way patients already access care. He discussed how even great tech fails if it’s too complex for real-world users, and used that lesson to showcase Sentara’s approach: define the purpose (for Sentara, it’s access), build a frictionless patient journey across every entry point (call center, nurse line, web, app), and invest heavily in the “after” (MA-led follow-up, referrals, medication questions) to make virtual care stick. He also walked through how Sentara uses virtual care strategically across models—from “Primary Care Lite” and hospital follow-ups to specialty programs—while balancing fee-for-service economics with value-based incentives like readmission reduction and ED avoidance.

“Regardless of how a patient starts their interaction with us, we are going to deeply integrate virtual care into that process, so that that call center agent, or that nurse, or that page on the website is simple to use and quickly navigates the patients to virtual care.”


Scaling In-Home Primary Care for the Most Complex Seniors
Katie Westman shared how Allina Health built and scaled an in-home primary care model for the top 1–2% most complex, frail seniors still living in the community – patients for whom both clinic-based primary care and traditional virtual care simply don’t work. She framed the “why” in a very human way: the physical and cognitive burden of getting to a clinic becomes an access barrier in itself, and in-home care is often the only realistic path to truly coordinated care. Katie walked through how Allina’s CoCare program combines a full interdisciplinary team (MD/NP, triage, RN care coordination, social work, pharmacy, care guides) to stabilize patients early, simplify care plans around patient goals, and reduce unnecessary utilization over time. Her patient story of “Carl” brought the model to life, showing how trust, environmental insight, and practical fixes (equipment, meds, affordability) can rebuild a relationship with care and restore quality of life, alongside measurable outcomes like reduced ED/hospital use and sustained satisfaction.

“Brick and mortar primary care works really well for a broad population of people. Virtual care works very well for a broad population of people. Yet we know we have a concentration of complex, frail seniors for which both brick and mortar and virtual don’t work well, and we just physically need to be in their home.”